



Surgical Technique for Creation of a Vaginal Canal (Neovagina)
Drs. Moore and Miklos utilize the laparoscopic modification of the Davydov procedure to create vaginas in women born without them (i.e. MRKH syndrome/vaginal agenesis) or in women that have a shortened vagina or painful vaginal cuff following surgery (such as hysterectomy). They complete more laparoscopic vaginal and pelvic reconstructive surgeries at their center in Atlanta than any other in the US and are considered world leaders in the field. They have women travel to Atlanta for their surgeries from all over the US and are invited to lecture and operate on their techniques throughout the world. They have pioneered many procedures that are considered standard of care in the field of Urogynecology today and complete all of their abdominal procedures laparoscopically (many of which are still done through large abdominal incisions at most other centers).
The Davydov Procedure is a surgical procedure used to create a full length vagina in young women that are born without a vaginal canal or lengthen the vagina in women with surgically shortened or scarred down vaginas. It is one of the most successful procedures described for this condition and utilizes the patient's own peritoneum (the cellular layer that lines the walls of the pelvis and the abdominal cavity) as the new vaginal canal. Dr. Miklos and Moore are able to use their expertise as laparoscopic pelvic/vaginal reconstructive surgeons to be able to complete the procedure laparoscopically, i.e. through tiny mini-incisions in the belly which makes it an outpatient type surgery. They operate off of large Hi-def TV screens that magnify the field allowing them to complete the surgery with more precision, better visualization, less blood loss and less complications versus traditional surgery. Recovery is rapid and the procedure carries the lowest risk of scarring down or losing the length created than any other procedure described to create vaginal length.
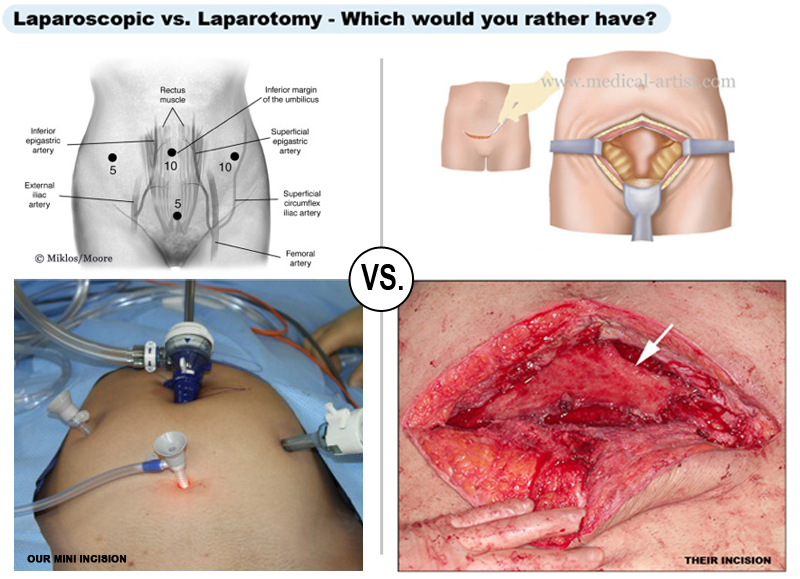
Many surgeons use an open abdominal incision (laparotomy) to complete these type of procedures. Dr. Miklos and Dr. Moore complete the Neovagina Procedure laparoscopically. See their incisions 'laparoscopic' (small incision) versus others 'laparotomy' (big incision). Which would you rather have?
Surgical Procedure
Dr. Miklos and Moore utilize their standard approach to laparoscopic pelvic reconstruction for the Laparoscopic Neovagina. Tiny incisions are made in the belly (one is hidden in the belly button) to allow access to the abdominal cavity. The procedure is completed with both a vaginal and laparoscopic approach, i.e. work is done from below vaginally, as well as above in the abdomen through the scope. Dr Moore and Miklos have a dedicated team of assistants to allow them to work together to accomplish the procedure. In the traditional approach to the surgery, approximately half of it is completed vaginally, however secondary to their expertise, they are able to complete most of it laparoscopically. The procedure typically takes them approximately 1 to 2 hours to complete and is completed in an outpatient type hospital setting.
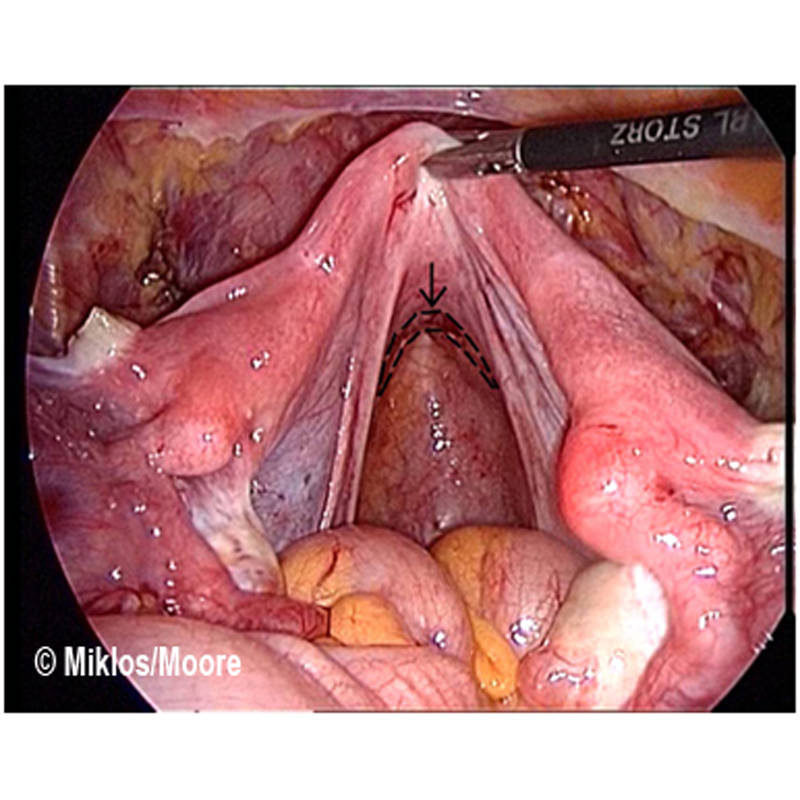
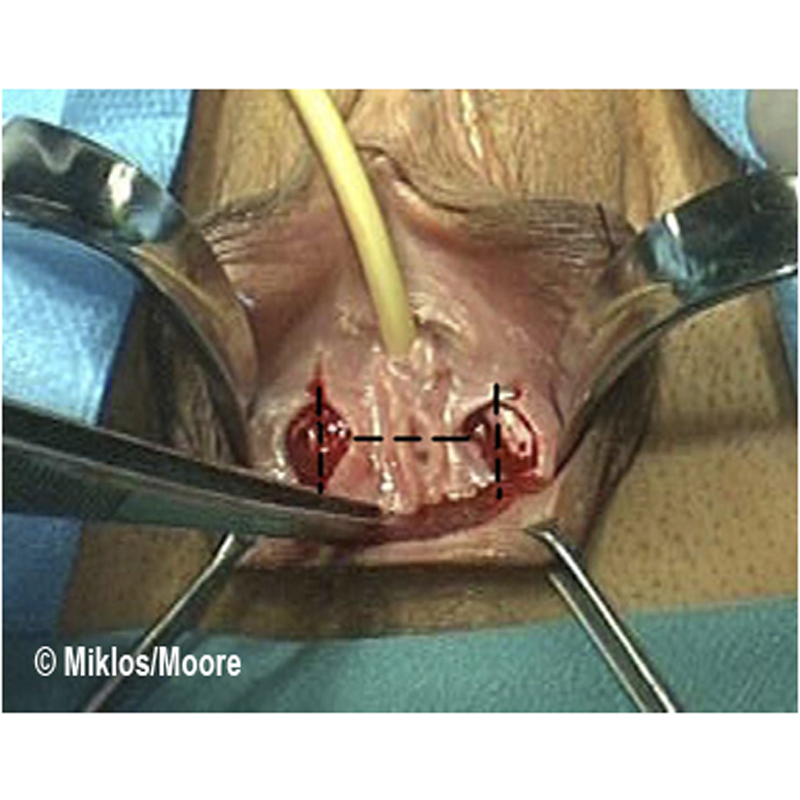
Figure 1 | Figure 2
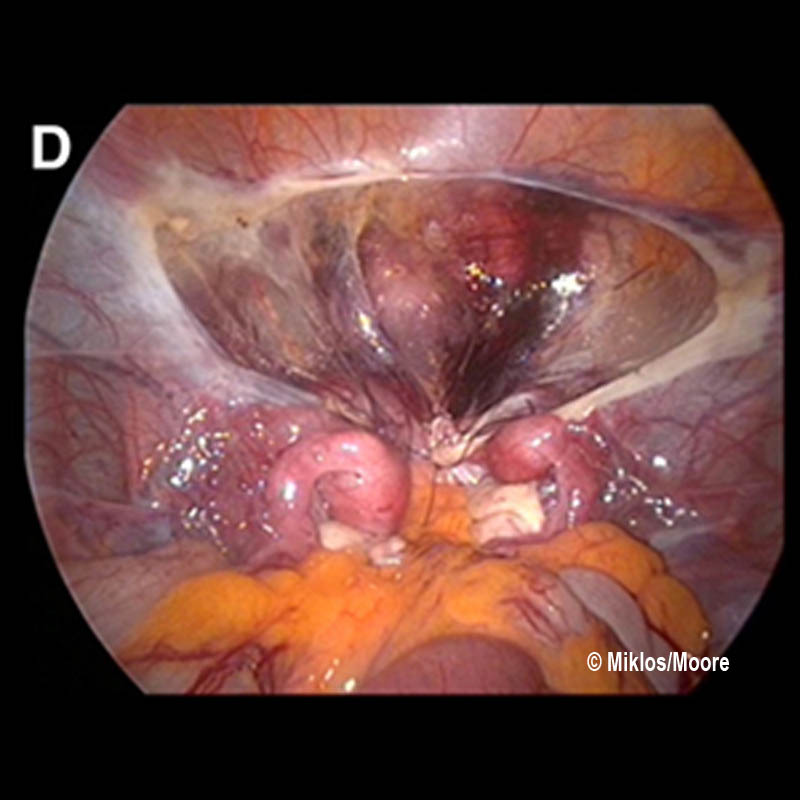
Figure 1 - Demonstrates the laparoscopic view down into the pelvis. The shiny covering of the pelvis (called peritoneum) will become the lining of the new vaginal canal. The arrow and dotted lines depict where the top of the vagina or dimple is located and that is the area that will be opened under direct visualization at the beginning of the procedure.
Once abdominal access is obtained, the vaginal dimple (or top of scarred down vagina in a shortened vagina) is opened to start the procedure. The most flexible part of the top of the vagina or dimple is located and with direct visualization from above laparoscopically, the vagina is opened with a large enough opening to accommodate two to three fingers.
Figure 2 - Vaginal photo of a MRKH patient with normal appearing external vagina, however one can visualize the vagina is very shortened and really just has a dimple where the vaginal canal should start. The dotted lines in the picture depict the incision that will be made to open up the top of the current vagina into the pelvis to enable the lengthening/neovagina procedure to be completed. The pelvic view of this incision can be seen above in Figure 1.
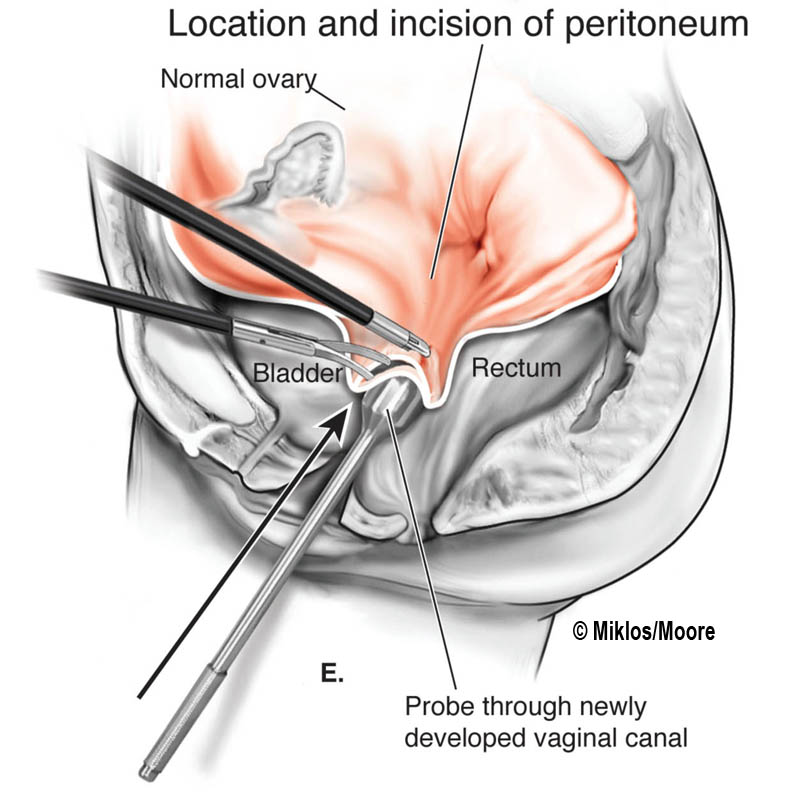
Figures 3A-E
The illustration (Figure 3 A-E) demonstrate where the incision is made in the vaginal dimple (becomes new vaginal opening) and then the probe is pushed up into the pelvis (Figure E) to incise the last layer (peritoneum).
Once the top of the vagina is opened into the pelvic cavity, the edges of the incised peritoneum is pulled down to the vaginal epithelium and the edges sutured together all around the opening. This is a step that can be completed vaginally, however Dr. Moore and Miklos typically will complete this step laparoscopically as well.

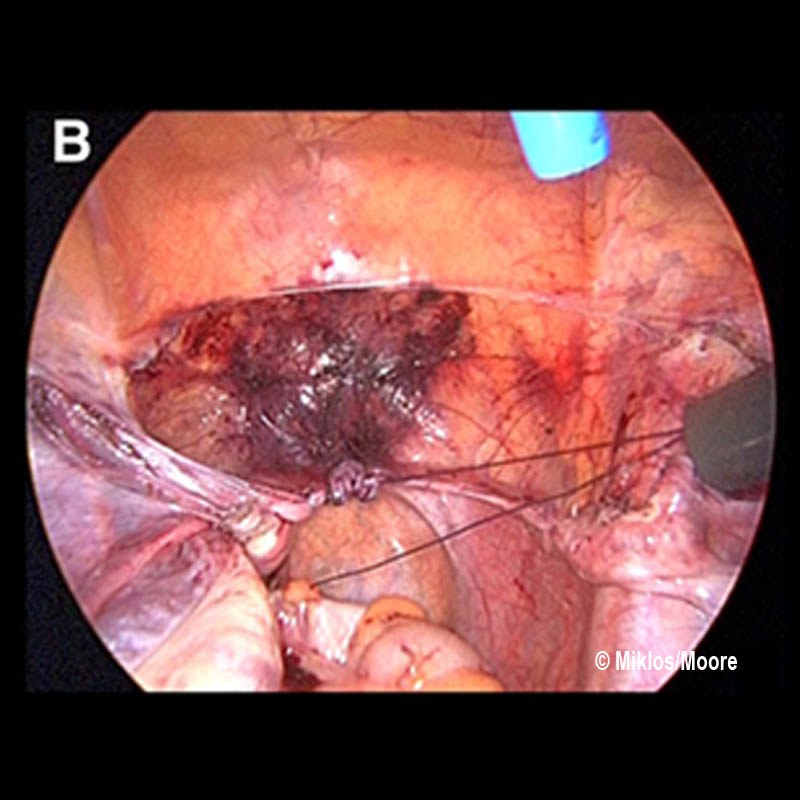
Figure 4A | Figure 4B
Figure 4A - The edges of the peritoneum can be visualized and these are advanced down and sutured to the edges of the opened vaginal skin edges.

Figure 5A
In Figure 5A there are NO raw surface edges exposed (these can be seen in Figure 4A). They are covered with the suturing of the peritoneum edges to the vaginal edges all the way around the circumference of the vagina and this minimizes risks of the vagina scarring down. This picture shows the lining of the new vagina very well, again note how there are NO raw surfaces and the peritoneal lining is very smooth and already completely epithelialized, i.e. it is not like a skin graft that has to heal or be accepted by the body.
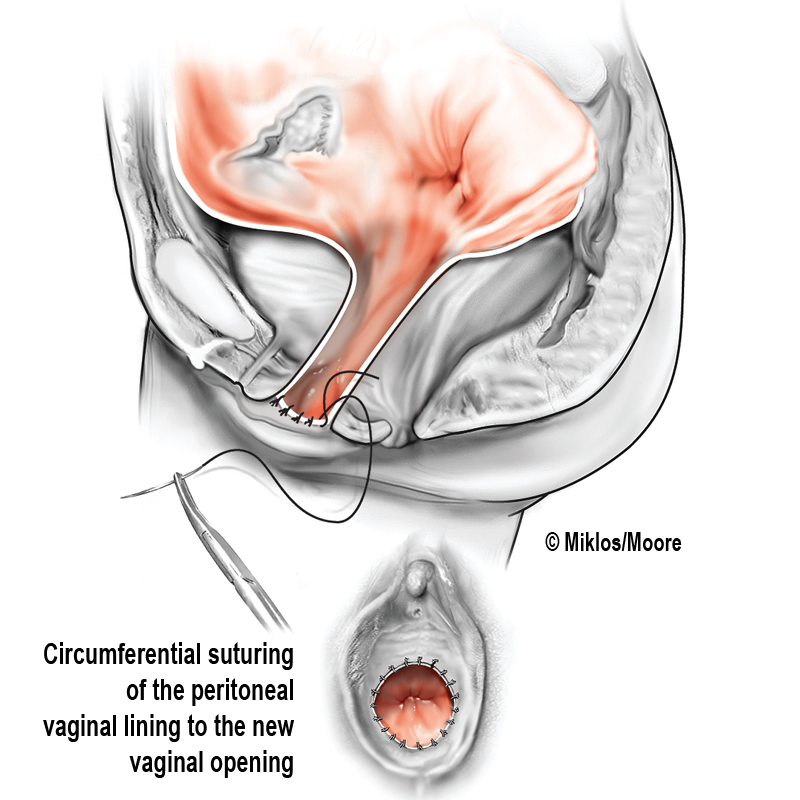
Figure 5b
The depth of the new vagina can be visualize in Figure 5B.
The new top or apex (cuff) of the vagina is now created laparoscopically. The vaginal length is marked from below and the peritoneum up higher in the pelvis is sutured in a purse string fashion to create the new upper portion of the vagina. Care is taken to avoid the ureters (the tubes going from the kidneys to the bladder) as well as the bowel.
Purse string sutures gathering together pelvic peritoneum – creating new top of the vagina
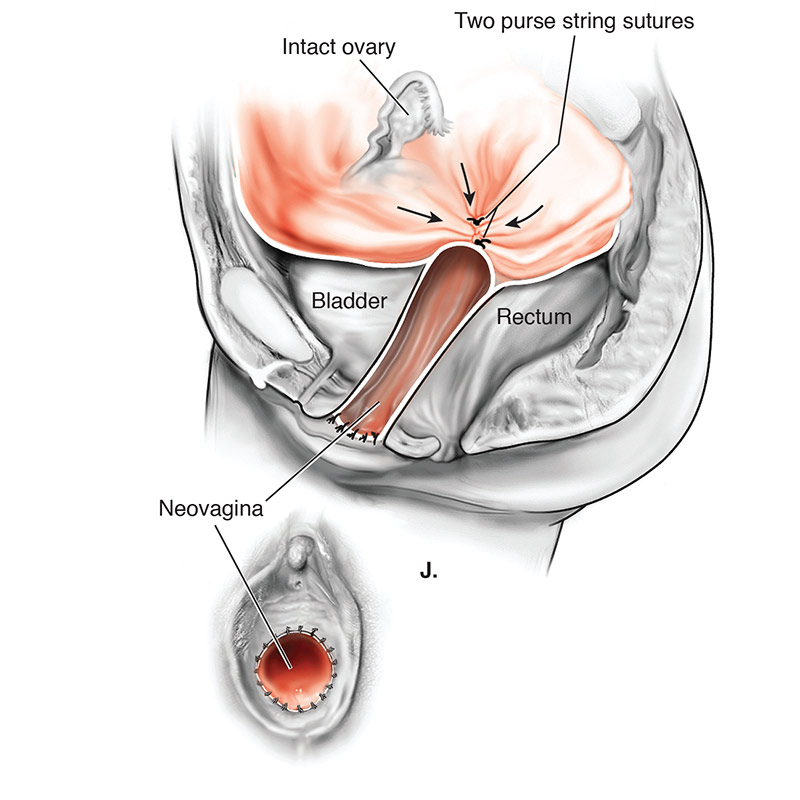
Figure 6A-D
Pictures source: Fedele. Am J Ob Gyn 2010.
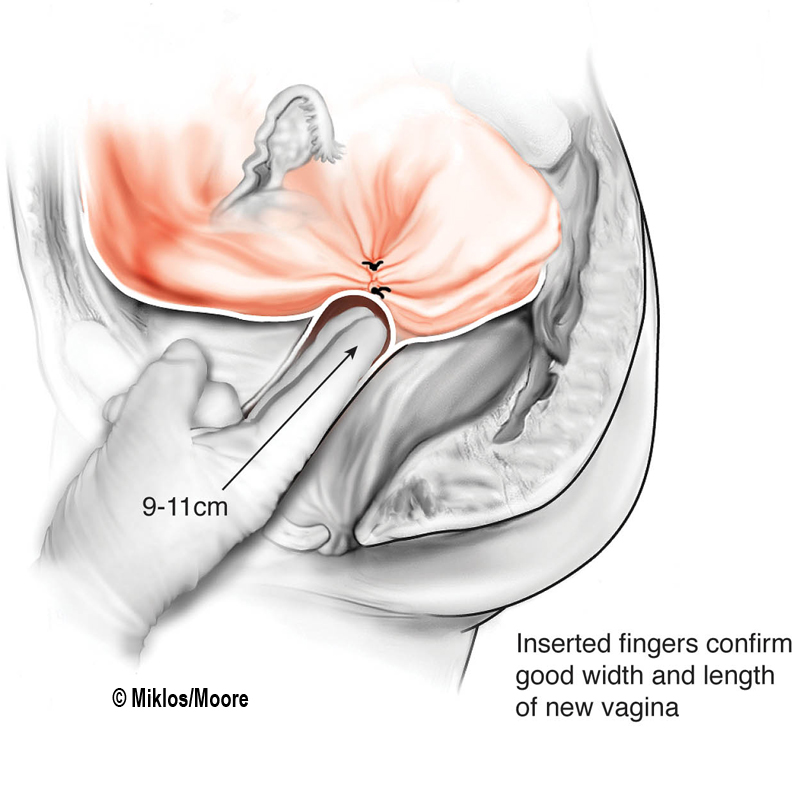
Figure 7 Before and After
Figure 7 (Before) shows patient with vaginal agenesis or very shortened vagina. Figure 7 (After) shows result after Laparoscopic Neovagina technique that utilizes the pelvic peritoneum to create a new vaginal canal. The shortened vagina is opened and the peritoneum from the pelvis is advanced down to the opening to create the lining of the new vaginal canal.